Article
‘Universal retraction suture’ for the overprojecting nasal tip
Abstract
Key Words: Nasal; Overprojecting; Overprojection; Projecting; Projection; Tip
The approach presented hereafter proposes the use of a suture technique that may be applied universally to any overprojected nasal tip, and that delivers a predictable and satisfactory result.
PROPER DIAGNOSIS OF NASAL TIP OVERPROJECTION: TRUE VERSUS PSEUDO
DIAGNOSIS OF NASAL TIP PROJECTION
DIAGNOSIS OF NASAL TIP PROJECTION
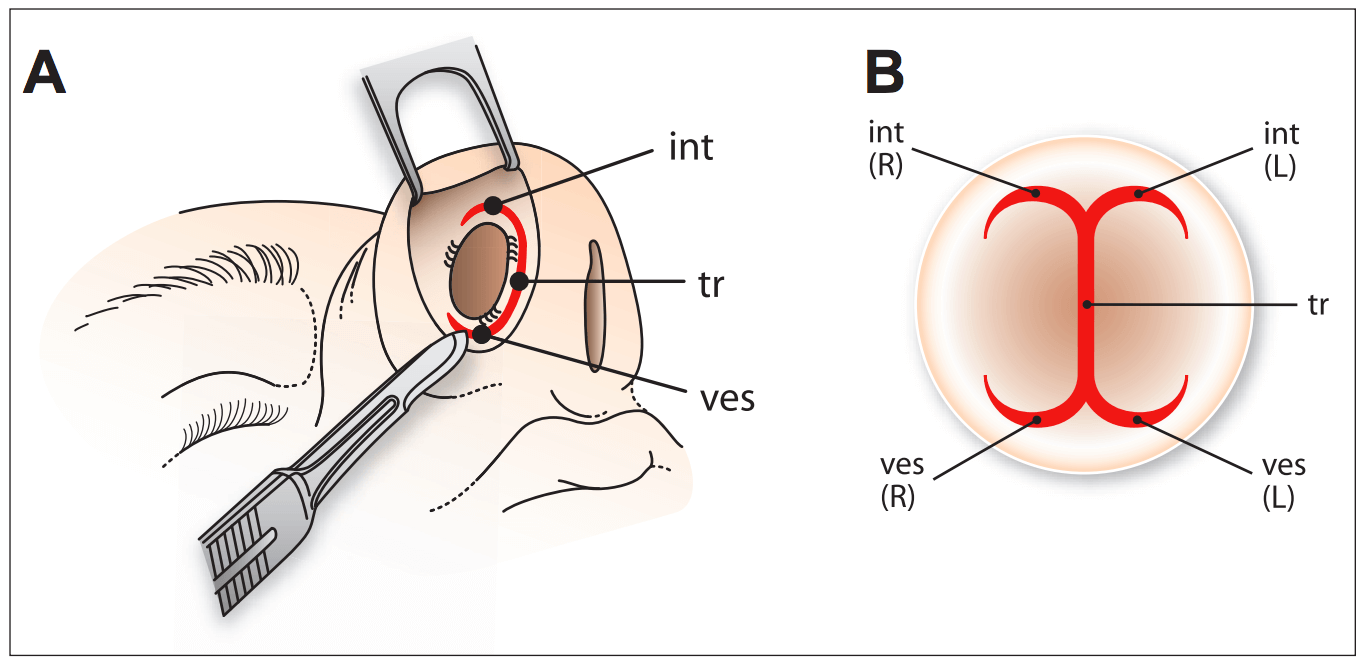
Figure 1) A‘Extended’ transfixion incision (tr). The tr is made through the membranous septum, separating the columella from the caudal septal border. The tr is then extended superiorly as right (R) and left (L) intercartilagenous incisions (int), then extended inferiorly as R and L vestibular incisions (ves). Therefore, the completed ‘extended’ tr (B) looks like the trunk of a palm tree (the original tr), with two branches from its top (the R and L int) and two roots from its bottom (the R and L ves)
THE UNIVERSAL RETRACTION SUTURE TECHNIQUE
Therefore, the ‘extended’ transfixion incision may be summarized as essentially a vertical line (the transfixion incision along the membranous septum), very similar to the trunk of a palm tree (Figure 1B). Superiorly, this line branches into two convex horizontal lines (the right and left intercartilaginous incisions), like two branches growing from the top of the palm tree. Inferiorly, the transfixion incision divides into two concave horizontal lines (the left and right vestibular incisions), like two roots growing from the bottom of the palm tree.
Now that the ‘extended’ transfixion is completed, the rhinoplasty procedure can proceed as usual with the tip alteration and the hump removal.
Nasal tip alternation
The usual technique needed for the correction of the alar cartilages (eg, resection and reshaping) may now be performed.
Dorsal hump removal
Resecting or rasping of the hump, as well as performing lateral osteotomies, may now proceed as usual. At this point, it is important for the surgeon to be very conservative in resecting the bony and lower cartilaginous dorsum, knowing that he can always return later to lower them further. This precaution is taken because the final level of the dorsum may only be decided with precision after finalizing the nasal tip projection with the ‘retraction suture’.
The ‘retraction suture’
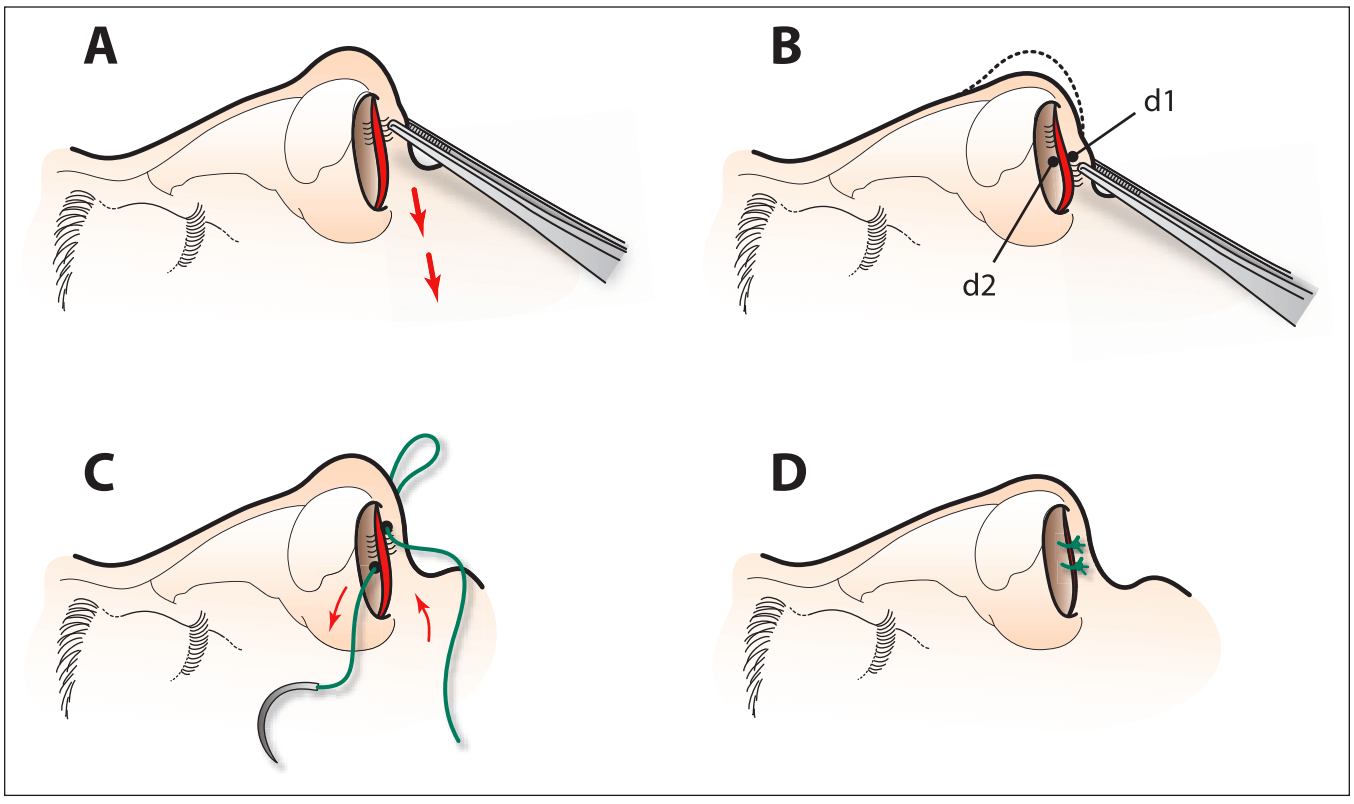
Using an Adson-Brown forceps, the surgeon catches the columella (Figure 2A) and moves it caudally (downward and posteriorly) until the tip projection is ideal. This manoeuvre gives the surgeon a precise idea of how much retrodisplacement is needed. With the columella pulled down to the desired level (Figure 2B), a marker pen is used to place a ‘dot’ at the midpoint of the ‘pulled’ columella (d1), and another ‘dot’ at the same level on the opposite caudal border of the septum (d2). The columella is then released. A suture is used (semipermanent 3-0 vicryl sutures are preferred) to approximate the two marked dots ‘d1’ and ‘d2’ (Figure 2C). The needle is first passed through and through (skin-medial crura-skin) at the dot ‘d1’ on the columella (Figure 2B and 2C). Then, the needle returns in the opposite direction through and through (mucosa-cartilage-mucosa) at the dot ‘d2’ on the caudal border of the septum (Figure 2B and 2C). As the suture is tied, the nasal tip moves caudally (inferiorly and posteriorly) to its ideal projection and is fixed in that position (Figure 2D). A second similar suture is then placed through both the caudal septum and columella, above or below the first knot, for further security (Figure 2D). The mucosa and skin edges above and below the two sutures are gently approximated with 5-0 chromic sutures.
Figure 2) The ‘universal retraction suture’ technique. A The surgeon catches the columella with forceps and moves it caudally until the tip projection is ideal. B Using a marker pen, a dot is placed on the midpoint of the height of the columella (d1) and another dot (d2) at the same level on the opposing caudal border of the septum. C A semipermanent suture is used to approximate the two ‘dots’. The needle passes through and through the columella and the septal border. D As the suture is tied, the nasal tip moves caudally and is fixed in an ideal projection. A second similar suture is then performed to secure the result
Sill resection of the nasal base (if needed)
In approximately two of three instances, retrodisplacing the nasal tip with the universal retraction suture leads to an unaesthetic flaring of the nostrils. In such cases, an alar base reduction, through the excision of a triangular piece of nostril base, is needed to narrow the nostrils. Figure 3 shows the successive surgical steps of the universal retraction suture technique.
PATIENT DATA AND RESULTS
DISCUSSION
CONCLUSION
Acknowledgments
REFERENCES
-
1. Soliemanzadeh P, Kridel RWH. Nasal tip overprojection: Algorithm of surgical deprojection techniques and introduction of medial crural overlay. Arch Facial Plast Surg. 2005;7:374–80.[PubMed]
-
2. Crumley RL, Lanser M. Quantitative analysis of nasal tip projection. Laryngoscope. 1988;98:202–8. [PubMed]
-
3. Tardy E, Walter MA, Patt BS. The overprojecting nose: Anatomic component analysis and repair. Facial Plast Surg.1993;9:306–16. [PubMed]
-
4. Goode R. A method of tip projection measurement. In: Powell S, Humphreys B, editors. Proportion of the Aesthetic Face. Thieme-Stratton; New York: 1984. p. 24.
-
5. Simons RL. Nasal tip projection, ptosis, and supratip thickening.J Ear Nose Throat. 1982;61:452–5.
-
6. Guyuron B, Ghavami A, Wishnek SM. Components of the short nostril. Plast Reconstr Surg. 2005;116:1517. [PubMed]
-
7. Ingels K, Orhan KS. Measurement of preoperative and postoperative nasal tip projection and rotation. Arch Facial Plast Surg. 2006;8:411–5. [PubMed]
-
8. Solomon P, Rival R, Mabini A, Boyd J. Transfixion incision as an initial technique in nasal tip deprojection. Can J Plast Surg.2008;16:224–7. [PMC free article] [PubMed]
-
9. Safian J. New York: 1935. Corrective Rhinoplastic Surgery. New York.
-
10. Lipsett EM. A new approach to surgery of the lower cartilaginous vault. Arch Otolaryngol. 1959;70:42–7. [PubMed]
-
11. Webster RC, Smith RC. Lateral crural retrodisplacement for superior rotation of the tip in rhinoplasty. Aesthetic Plast Surg.1979;3:65–78. [PubMed]
-
12. Parkes MH, Kanolia R, Kern EB. The universal tip: A systemic approach to aesthetic problems of the lower lateral cartilages. Plast Reconstr Surg. 1988;81:878–90. [PubMed]
-
13. Conrad K. Nasal tip reduction: Predictable part of rhinoplasty. J Otolayngol. 1981;10:420. [PubMed]
-
14. Papanastasiou S, Logan A. Management of the overprojecting nasal tip. A review. Aesthet Plast Surg. 2000;24:353–6. [PubMed]
-
15. Foda HMT. Alar setback technique: A controlled method of nasal tip deprojection. Arch Otolaryngol. 2001;127:1341–6.[PubMed]
-
16. McCullough E, Mangrat D. Systemic approach to correction of the nasal tip in rhinoplasty. Arch Otolaryngol. 1981;107:12–6.[PubMed]
-
17. Ghavami A, Janis JE. Tip shaping in primary rhinoplasty: An algorithmic approach. Plast Reconstr Surg. 2008;122:1229–41.[PubMed]
-
18. Kridel RWH, Konior RJ. Domes truncation for management of the overprojected nasal tip. Ann Plast Surg. 1990;24:385–96.[PubMed]